
AREFEH RAVANBAKHSH
Clinical history
A 12-year-old female spayed German Shepherd presented to their veterinarian for examination of a mammary mass. Approximately 11-months earlier, the patient had multiple mammary masses removed. Histological examination of the previous mammary masses had revealed mixture of benign and malignant mammary tumours.
Approximately 10-months following surgery to remove the initial mammary masses, the patient developed another mammary lesion. On presentation the mass was described as firm, diffuse, painful on palpation, and measuring approximately 10cm x 2cm in size.
Fine-needle-aspirates of the mammary mass were performed and the smears were submitted to Gribbles for cytology. An EDTA sample and fresh blood smear was also submitted for a full CBC.
Haematology results
CBC revealed a neutrophilia (30.5 x 109/L; reference interval 3.6-11.5 x 109/L), left shift (bands 6.5 x 109/L; RI 0-0.5 x 109/L), and monocytosis (4.7 x 109/L; RI 0.2-1.5 x 109/L) all consistent with a marked inflammatory leukogram. There was a stress lymphopenia (lymphocytes 0.4 x 109/L; RI 1.0-4.8 x 109/L), and few reactive lymphocytes. The erythroid mass was within normal range, HCT 0.42 (RI 0.37-0.55 L/L). Platelet mass was also within normal limits.
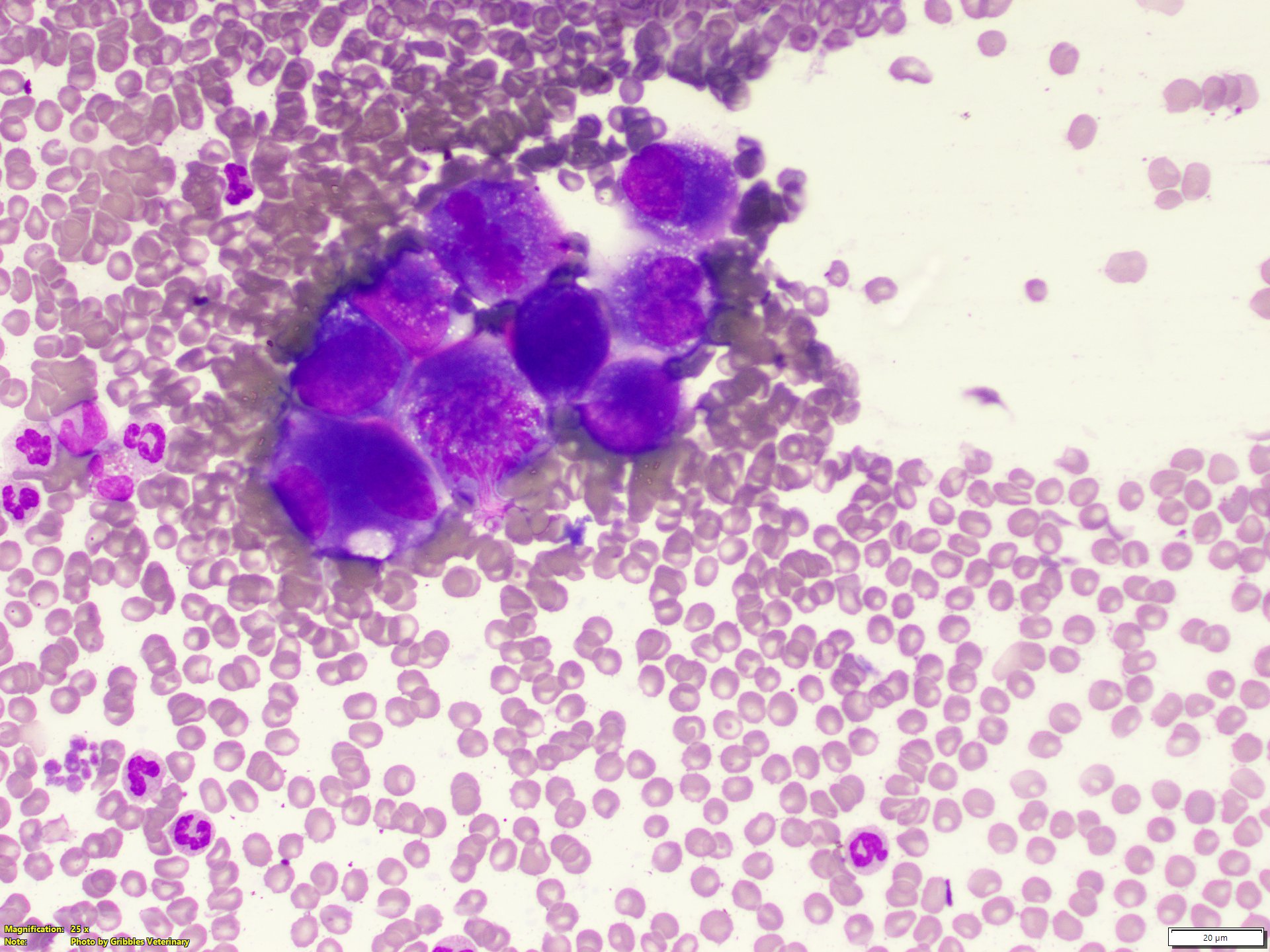
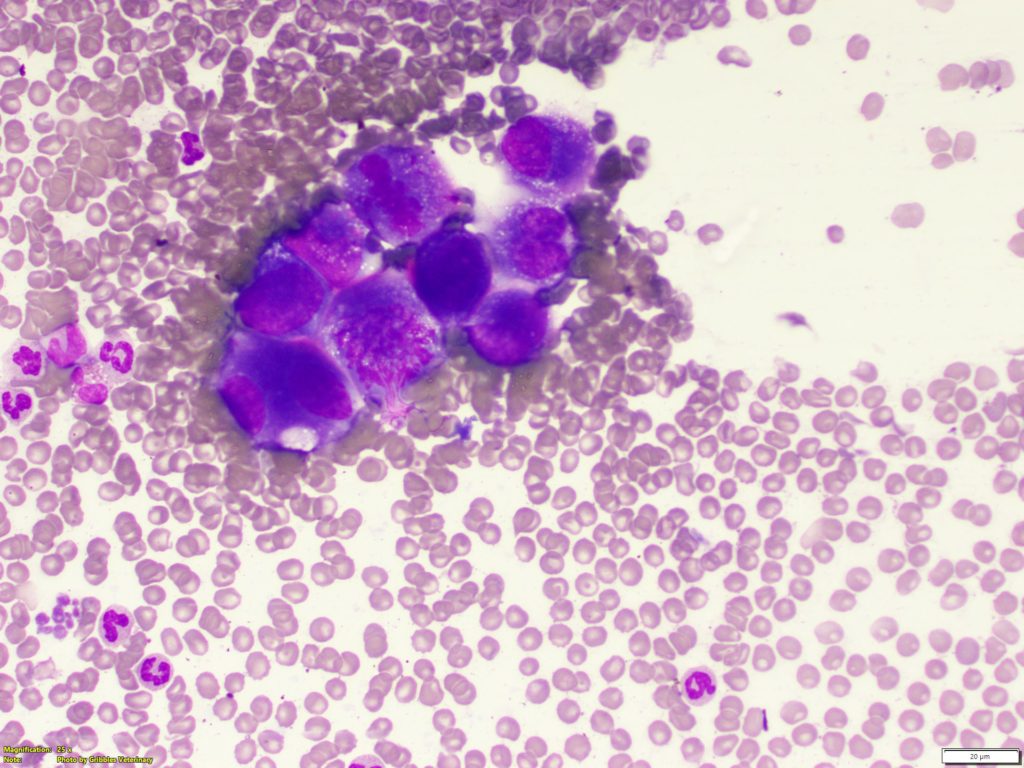
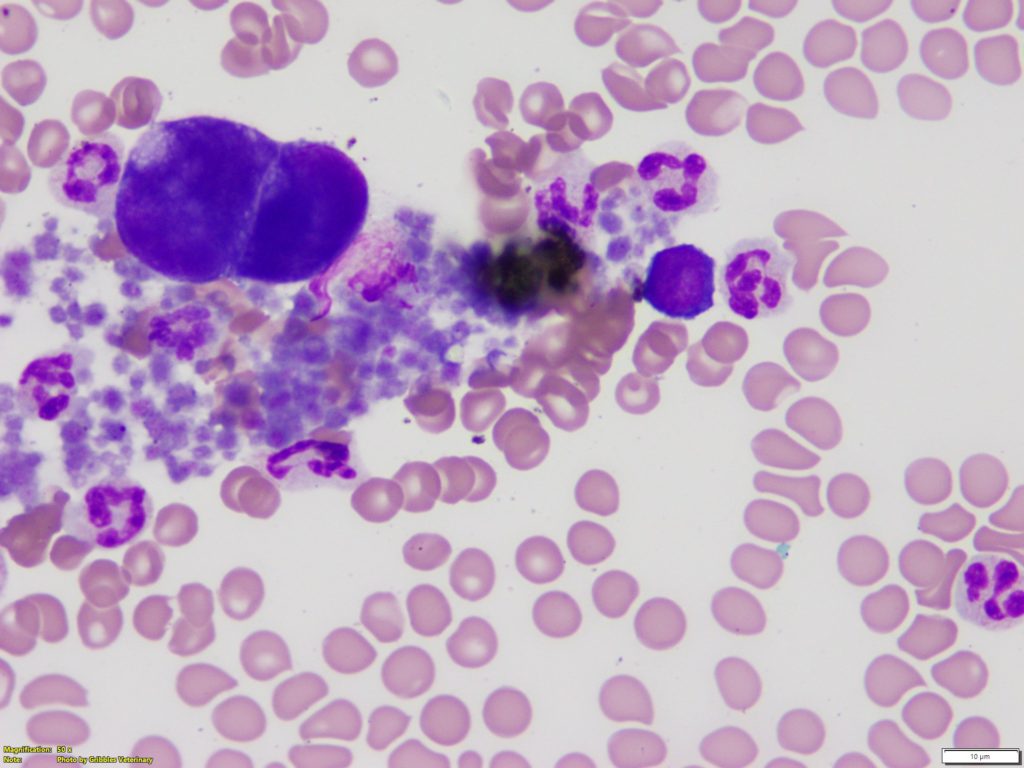
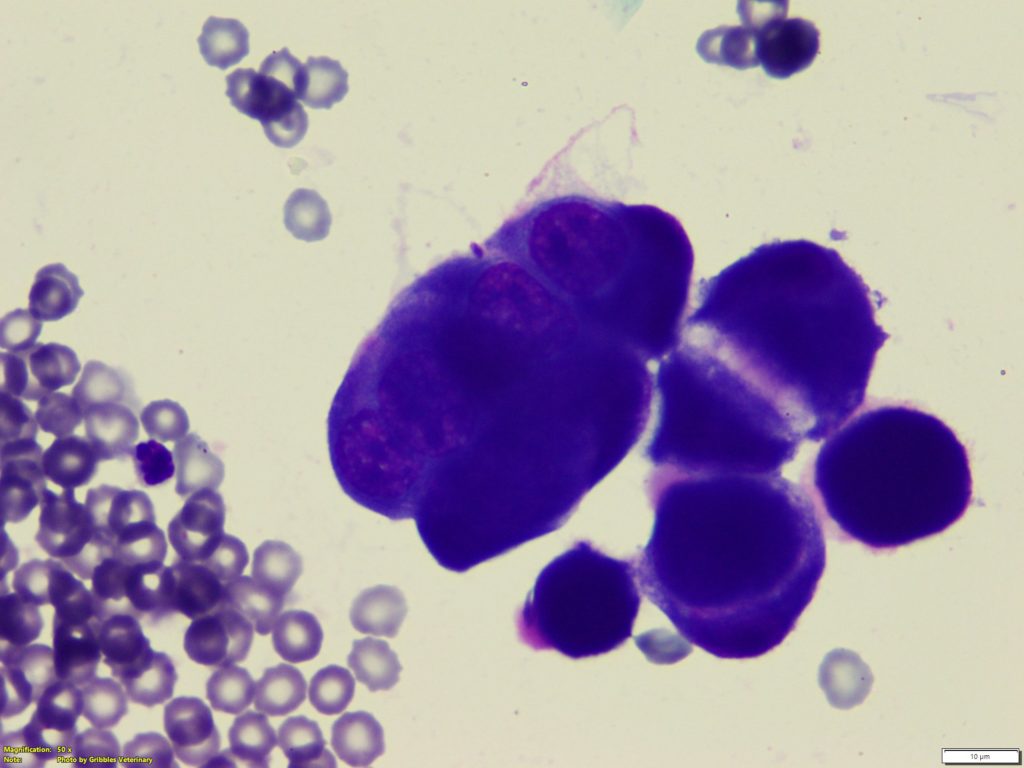
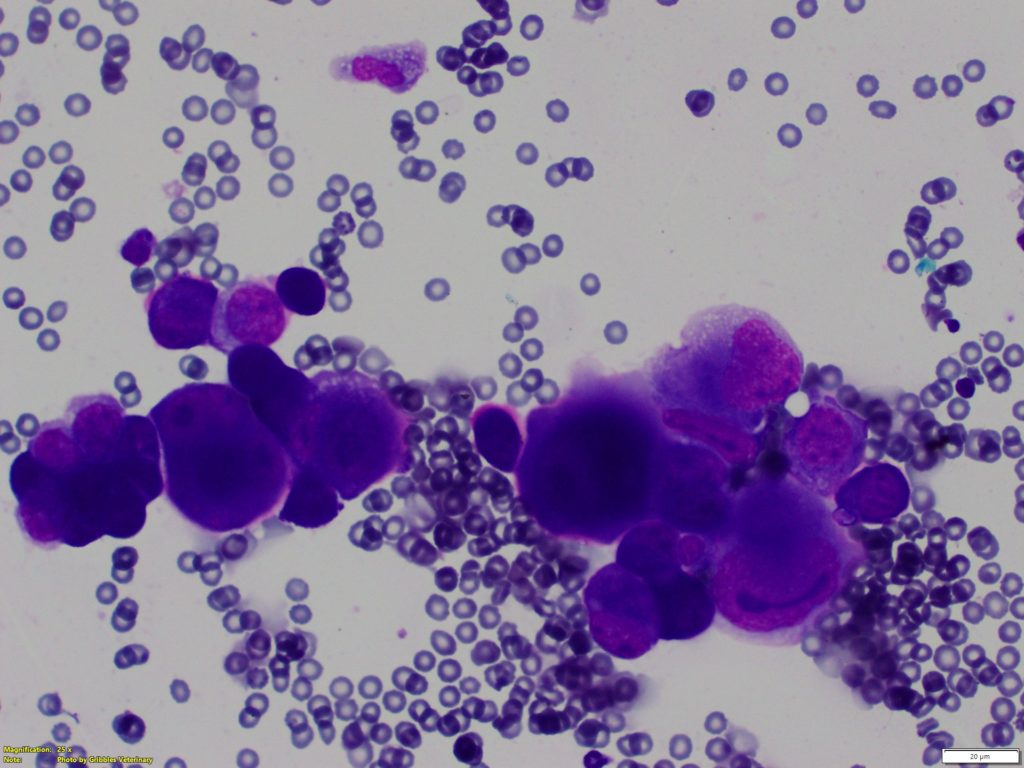
On blood smear review a population of atypical cells were noted, mostly on the feather edge of the blood smear (Figures 1 and 2 A+B). The atypical cells were large rounded to polygonal, had small to moderate amount of basophilic to deep basophilic cytoplasm that were variably vacuolated. Nuclei were paracentral to eccentric, round, oval, or indented with coarse chromatin pattern and one to multiple distinct and at times prominent nucleoli. The atypical cells were noted individually or forming small cohesive clusters.
Cytology of mammary mass
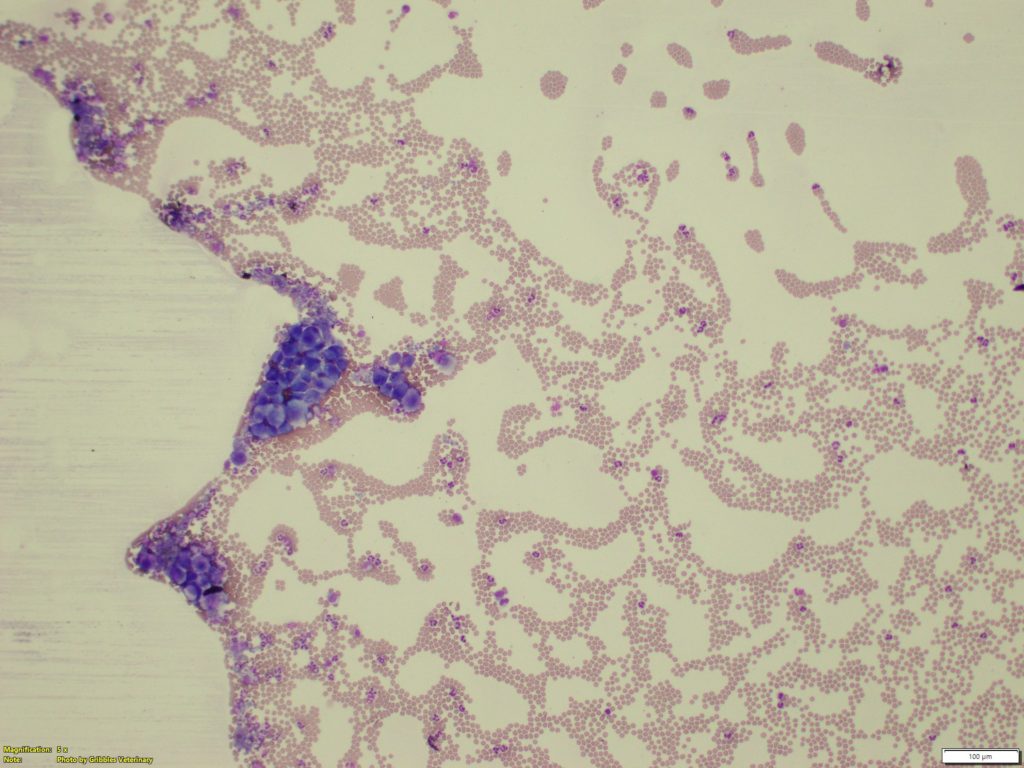
The sample was well preserved and highly cellular with mild to moderate blood contamination (Figures 3 A + B). A moderately to markedly atypical epithelial cell population was noted in variably sized clusters as well as scattered individually. Few clusters were associated with scant amount of pink proteinaceous material. The epithelial cells were polygonal to round and had small to moderate amount of deep basophilic cytoplasm, variably distinct cell junctions, and some had a variable degree of clear vacuolation. Nuclei were paracentral to eccentric, round, oval, or indented and contain coarse chromatin with one to few prominent, round, oval, or irregular nucleoli. There was moderate to marked anisokaryosis, and frequent bi- or multi-nucleated forms and evidence of nuclear moulding and cell crowding. Occasional mitotic figures were noted some of which displayed asymmetrical mitosis. Non-degenerate neutrophils and macrophages were mildly increased.
Diagnosis
Malignant neoplasia, most consistent with carcinoma, with evidence of circulating neoplastic cells.
Discussion
Cytology can be a great diagnostic tool to further investigate if a mass in the region of the mammary glands is of mammary origin, or due to other pathology in the vicinity of the mammary glands (example a mast cell tumour or abscess in close proximity to the mammary chains). Cytology alone however can be poorly predictive of biological behaviour (benign vs malignant) when it comes to mammary tumours, and histopathology is needed to further differentiate mammary tumours.
Presence of circulating neoplastic cells with morphology which mirrored that noted in the mammary mass cytology, marked cytological atypia of the majority of exfoliated epithelial cells, and history of previous mammary carcinoma, all helped provide clues to support diagnosis of carcinoma in this case.
This case highlights the importance of including a blood smear examination as part of a haematology work-up (CBC). If only the machine generated values were assessed without a concurrent blood smear examination, the presence of circulating neoplastic cells would not have been detected.
In canine mammary carcinomas, detection of circulating tumour cells is a rare finding.1 In human breast cancer patients, the presence of circulating tumour cells is prognostically significant.2 Circulating tumour cells in human patients indicates increased risk of metastasis and higher numbers of circulating neoplastic cells have been inversely associated with patient survival.3
Thank you to Dr. Sophia Xu and Forrest Hill Veterinary Clinic for submitting this interesting case.
References:
1. Piane L. et al. What is your diagnosis? Abnormal cells on a blood smear from a dog. Vet Clin Pathol. 3:461-2, 2014
2. Jaillardon L. et al. Mammary gland carcinoma in a dog with peripheral blood and bone marrow involvement associated with disseminated intravascular coagulation. Vet Clin Pathol. 2:261-5, 2012
3. Park H, Brown SR, and Kim Y. Cellular Mechanisms of Circulating Tumor Cells During Breast Cancer Metastasis. Int J Mol Sci. 21:5040, 2020.