
We present two haematology cases with similar findings.
Case 1
An 11-year-old Labrador presented with generalised splenic enlargement, pale mucous membranes, decreased appetite and a small amount of weight loss.
CBC revealed a marked leukocytosis and moderate non-regenerative anaemia, with haemoglobin 79 g/L, HCT 0.25 L/L and WBC 242 x109L. Neutrophils were only slightly increased (12.1 x109/L) however the lymphocytes were markedly increased with 229.9 x109/L.
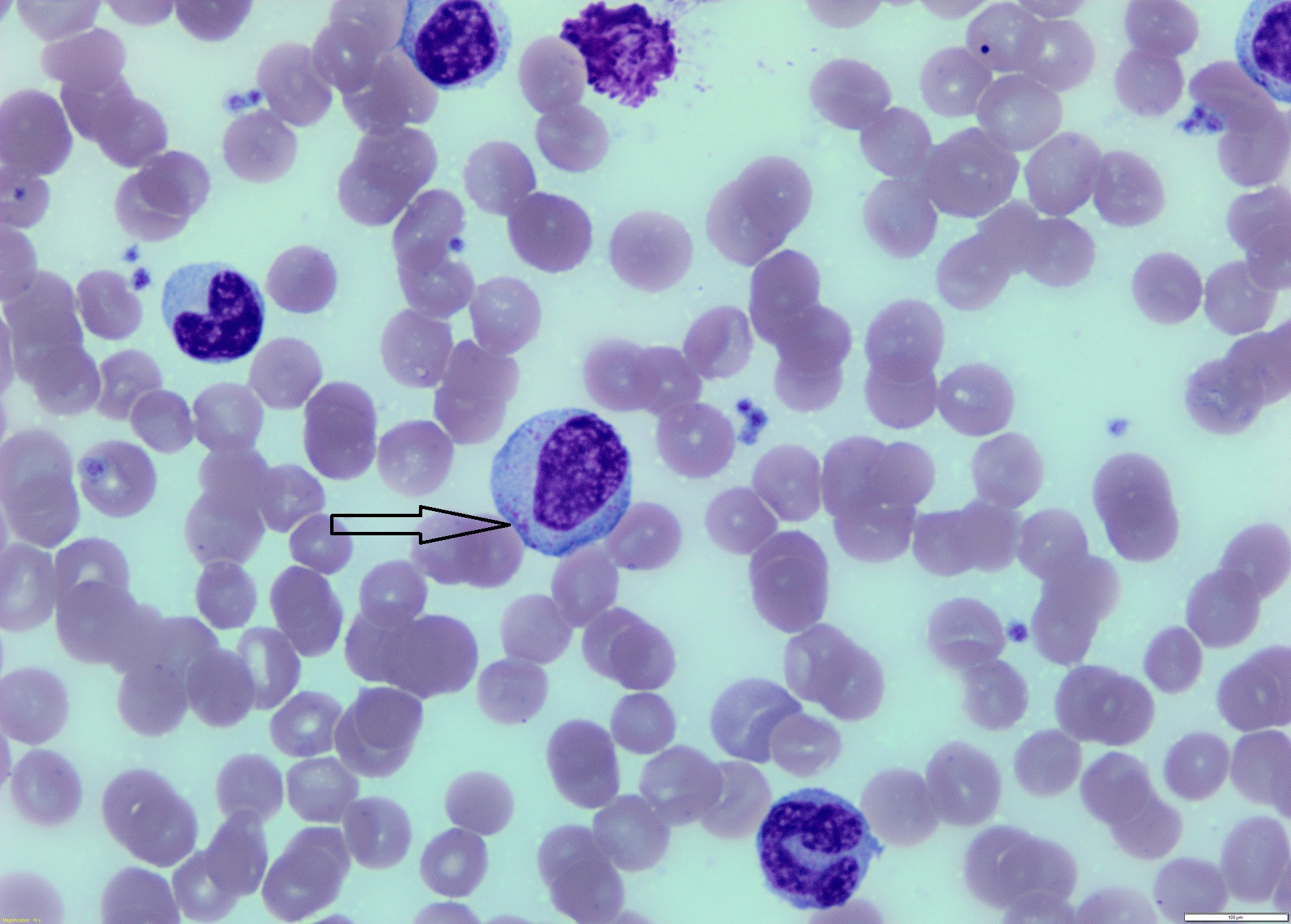
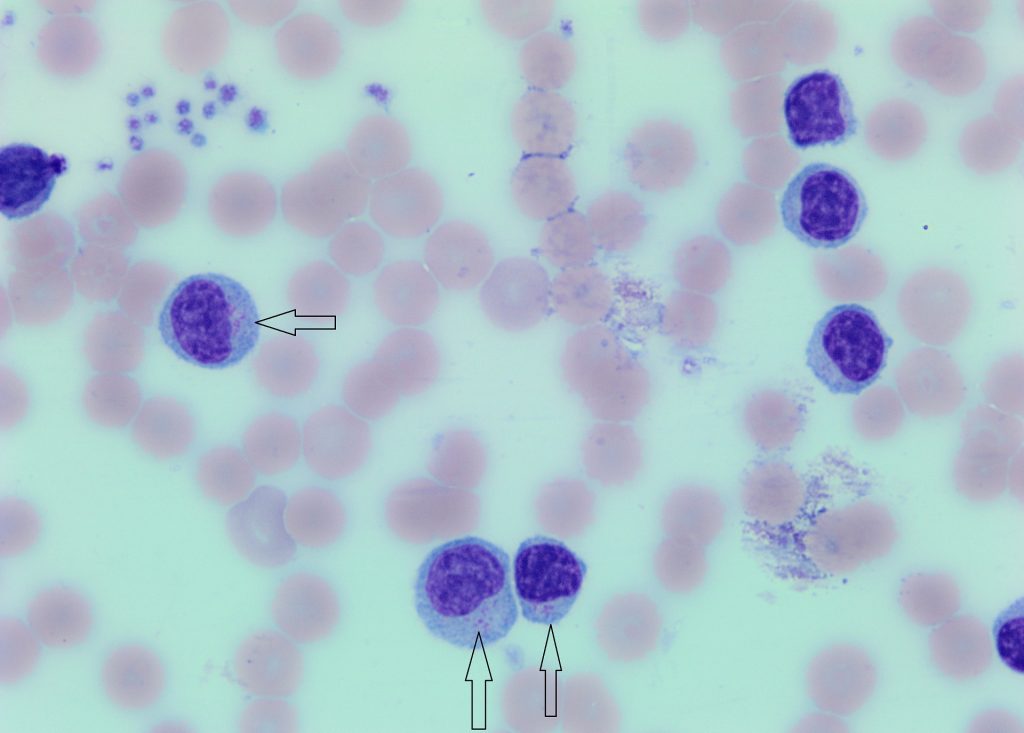
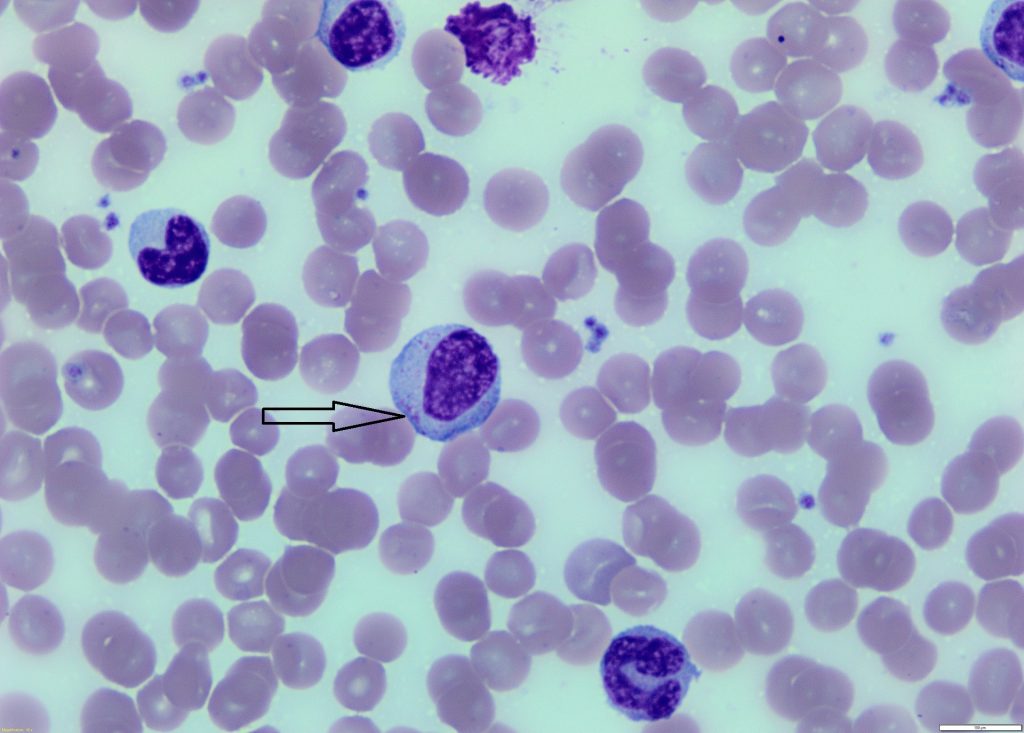
Most of the lymphocytes were small to medium size, with round to slightly indented nuclei approximately 2-3x the size of RBCs. They had a clumped chromatin pattern, medium blue cytoplasm with azurophilic granules. Occasional medium to large lymphocytes were also seen, with nuclei 4x the size of RBCs, reticular chromatin pattern and medium blue cytoplasm with azurophilic granules.
Case 2
A 12-year-old Golden Retriever presented with haematochezia, weight loss and lack of appetite.
CBC revealed a marked leukocytosis and lymphocytosis with a WBC count of 118.8 x109/L. Lymphocytes were markedly raised at 90.3 x109/L and neutrophils and monocytes also raised at 22.6 and 5.9 x109/L respectively.
Most of the lymphocytes were medium size, with nuclei 2-3x the size of RBCs, and a medium N/C ratio. Nuclei were round to slightly indented, contained reticular chromatin pattern and abundant pale blue cytoplasm with azurophilic granules.
Diagnoses:
Chronic lymphocytic leukaemia (granular lymphocyte morphology).
Discussion:
Leukaemia is defined as the presence of neoplastic cells of hematopoietic origin in the blood and/or bone marrow. Chronic leukaemia indicates that the cell type involved (ie lymphoid in the reported cases) are mature in morphology. In chronic lymphocytic leukaemia (CLL) the lymphocytes are small to intermediate in size with clumped chromatin and indistinct nucleoli (vs acute leukaemia with large immature mononuclear cells, with fine sand-like chromatin patterns and often prominent nucleoli). In general chronic leukaemias are indolent diseases that have a prolonged natural course, however this is dependent upon the time the leukaemia is first detected.
Granular lymphocytes (GL) are characteristic, in that small to large numbers of fine to large magenta granules can be detected in the cytoplasm of the lymphocytes. It should be noted that some in-house quick stains may not pick up some of the more finer granules in GL. GL may be seen in low numbers in circulation in healthy dogs and cats, but may increase in number with antigenic stimulus and chronic inflammation. When numbers are markedly increased and cytomorphology is monomorphic, we suspect a neoplastic proliferation.
Leukaemia with GL morphology has previously been called LGL (Large Granular Leukaemia or Large Granular Lymphocytes), although we are moving away from this confusing term, especially for cases of CLL. CLL with GL morphology is most commonly identified in large breed older dogs (average age at diagnosis is around 10 years) and often originates from the spleen (and occasionally the intestinal tract). Anaemia is a common concurrent finding.
The dog in Case 2 was treated with chlorambucil and prednisone. We received bloods for repeat CBCs 3- and 16-months after the initial CBC. The WBC had decreased to 43.3 x109/L after 3 months and remained stable at the 16-month check. The dog has however developed a mild progressive anaemia, which was showing signs of regeneration at the last CBC.
No further samples have been received from the dog in Case 1.
THANK YOU TO FAMILY VETS, ROTORUA AND CAREVETS CHARTWELL FOR THESE INTERESTING CASES.