

Bernie Vaatstra
Many vets will be able to recount removing astonishingly large splenic masses from dogs. Splenectomy may occur in the context of an emergency – after splenic bleed or torsion, for example – or after detection of an incidental mass on palpation.
Since it is difficult to determine malignant potential based on gross appearance alone, these spleens often end up in the laboratory for processing. Large splenic samples have areas of coagulated blood and necrosis, are densely cellular and slow to fix in formalin, and are messy to process. They are generally challenging for pathologists and histology technicians and care is required in case selection and sample submission.
So, what are the differentials for these large splenic masses? A survey of 83 splenic masses received through one of our laboratories over the course of two years revealed the diagnoses outlined in Table 1.
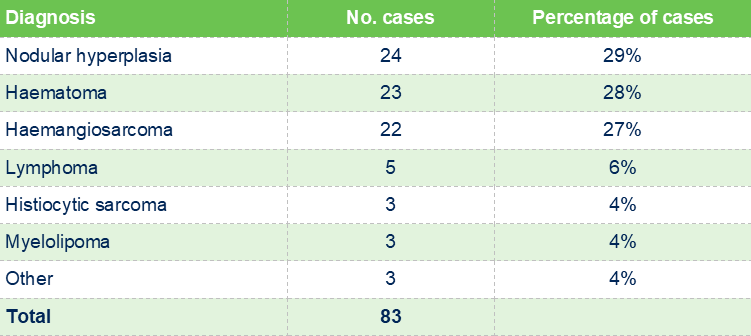
Of these differentials, nodular hyperplasia, haematoma and haemangio-sarcoma are clearly most commonly encountered, with the others being
uncommon. The spleen may also harbour metastatic tumours such as mast cell tumour, melanoma, multiple myeloma, and neuroendocrine carcinoma.
The gross appearance of the splenic mass may suggest more likely differentials but is never entirely reliable. A large solitary mass may be more likely to be nodular hyperplasia nodule, stromal sarcoma, haematoma, or myelolipoma. Scattered smaller nodules could be lymphoma, metastatic neoplasia, disseminated vascular neoplasia, or histiocytic sarcoma, but again, could also be multiple hyperplastic nodules. Multiple irregular, ragged dark red masses would raise concern for haemangiosarcoma. A diffusely enlarged spleen suggests conditions such as haemolytic anaemia, lymphoproliferative disease, histiocytic sarcoma, EMH, and splenitis.
Given the variable gross appearance and differing prognoses of splenic masses, histopathology remains an essential component in diagnosis and management. Ideally, the entire spleen should be fixed for several days in an appropriate quantity of 10% neutral buffered formalin (10:1 formalin to tissue ratio, or as close to as practicable). To aid fixation, the spleen can be partially bread-loafed (Figure 1). The fixed spleen can then be removed from the formalin, wrapped in gauze or paper towels, and placed in sealed, zip lock bags within an outer sturdy container containing absorbent material.

If it is impractical to fix the entire spleen, 4-6 samples should be collected from the mass/spleen interface since that tends to be the region where any neoplastic cells are best preserved and most plentiful.
Histopathology will often provide a definitive diagnosis but has some limitations. For masses complicated by necrosis and haematoma, areas of malignancy can be obscured. In addition, nodular lesions often have mixed cell populations – lymphoid, histiocytic or stromal – and one or more of these populations may be malignant (Sabattini et al. 2022). Further, while we endeavour to select the most representative portions of a splenic mass for processing, it is not possible to exclude the possibility of missing a diagnostic focus given histological sections generally consist of roughly 40 x 20mm of tissue measuring up to 5 µm thick. As an example, one study of dogs with splenic haematomas found that up to 10% may have had undetected malignancy based on clinical follow up (Patten et al. 2016). The histological diagnosis should therefore always be interpreted alongside relevant clinical findings, haematology and biochemistry.
References:
> Patten SG, Boston SE, Monteith GJ. Outcome and prognostic factors for dogs with a histological diagnosis of splenic hematoma following splenectomy: 35 cases (2001-2013). Can Vet J. 57:842-6, 2016.
> Sabattini S, Rigillo A, Foiani G, Marconato L, Vascellari M, Greco A, Agnoli C, Annoni M, Melchiotti E, Campigli M, Benali SL, Bettini G. Clinicopathologic features and biologic behavior of canine splenic nodules with stromal, histiocytic and lymphoid components. Front Vet Sci. 12:9:962685, 2022.